Inhaltsverzeichnis | Sommaire
Patient safety and error management in healthcare are key concerns in modern healthcare. Every incident, every mistake that harms a patient is one too many. However, mistakes are inevitable in human action, including in the Swiss healthcare system. The decisive factor is how organizations react to this: with a blame culture that sanctions individuals, or through systematic analysis that optimizes processes and increases patient safety? According to estimates, 2000 to 3000 patients die every year in this country from avoidable errors and complications (SRF, 2020). Many of these tragic incidents could be prevented if an open and learning-oriented safety culture were established. This is exactly where the concept of Just Culture – often translated as a culture of justice – comes in. It offers a differentiated approach to overcoming the blame culture, promoting safety, distributing responsibility fairly, and establishing a culture of trust and learning. In this blog article series, we will take a detailed look at the concept of Just Culture, starting with the basics and error management in healthcare in this first part.
What is Just Culture and how does it promote error management in healthcare?
At its core, Just Culture shifts the focus away from the question “Who made the mistake?” to “What went wrong and why?”. It is an approach that views errors not primarily as individual failures, but as the result of weaknesses in the system – be it in processes, technologies or organizational structures (Reason, 1997). A Just Culture recognizes that even competent and committed professionals can make unintentional mistakes. However, that doesn’t mean that Just Culture is a “no-blame” culture where no one is held accountable. Rather, it is about balanced accountability (Boysen, 2013). A clear distinction is made between:
- Human Error: Unintentional actions, such as a slip of the tongue, oversight, or unintentional slipping. The response to this is comfort, support, and most importantly, learning from the incident to improve the system.
- At-Risk Behavior: A deliberate decision to take a shortcut or deviate from a rule, underestimating the risk or seeing it as justified. This is where coaching, root cause analysis and system adjustments are needed.
- Reckless behavior: A deliberate disregard for a significant and unjustified risk. This is rare, but requires consistent action, including disciplinary measures (Marx, 2001).
The key difference is that the response is tailored to the behavior and circumstances, not just the outcome. A functioning Just Culture creates an atmosphere of trust and psychological safety. Employees feel encouraged to openly report errors, near misses, and safety concerns without automatically fearing sanctions (Boysen, 2013, Dekker, 2012). This openness is the basis for organizational learning and the continuous improvement of patient safety. Error management in healthcare is a critical factor in fostering such a safety culture.
A brief review: From Reason to Marx to Dekker and their importance for error management in the healthcare sector
Just Culture’s roots lie deep in safety research, particularly in high-risk industries such as nuclear energy and aviation, where failure analysis has helped improve safety for decades. Psychologist James Reason is considered one of the most important thought leaders. His Swiss cheese model (1990) illustrates how errors arise from the interaction of several vulnerabilities (Reason, 1990). In his seminal book “Managing the Risks of Organizational Accidents” (1997), he described Just Culture as an essential component of a broader safety culture. Reason argued that a Just Culture is necessary to build the trust that is essential for a functioning reporting culture – a culture in which security incidents are reported so that lessons can be learned.
The engineer and lawyer David Marx made a significant contribution to transferring the concept of Just Culture specifically to healthcare. His report, “Patient Safety and the ‘Just Culture’: A Primer for Health Care Executives” (2001), helped establish the principles in the medical context. Marx emphasized the need to resolve the tension between system responsibility and individual responsibility, developed models for analyzing human behavior in the work context and, with Just Culture, created the framework for a fair, learning-oriented error culture that distinguishes between human error, risky and reckless behavior.
Further impulses were provided by the social scientist Sidney Dekker, who developed the idea of a “Restorative Just Culture”. This approach emphasizes not only the analysis of mistakes and the fair allocation of responsibility, but also the needs of the injured parties (patients, relatives, but also employees involved) and the assumption of responsibility for reparation and healing (Dekker, 2012). Healthcare error management benefits from these approaches and helps improve patient safety.
Visualizing errors: The Swiss cheese model
Another important concept that is closely linked to Just Culture is the Swiss Cheese Model developed by James Reason. This model illustrates how accidents typically occur in complex systems (Reason, 1990, 1997). Various safety barriers of an organization – such as guidelines, technology, training, checklists – are represented as slices of a Swiss cheese. Each disc has holes that represent weak points or potential sources of failure in that specific barrier that are constantly changing in size and position.
According to this model, an accident or a serious incident occurs when the holes of several cheese slices (safety barriers) happen to lie on top of each other for a moment. This creates a “trajectory of accident opportunity” that allows a hazard to penetrate all lines of defense and lead to damage (see figure from bundesaerztekammer.de). The model distinguishes between:
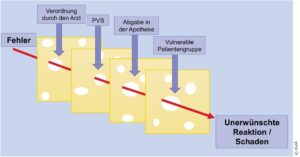
- Active Failures: Unsafe actions
that lead directly to the incident (e.g. medication mix-up). - Latent Conditions: Hidden vulnerabilities in the system that often go unnoticed for a long time before contributing to an incident (e.g. similar-looking medication packaging, lack of staff, unclear processes, inadequate training).
The Swiss cheese model helps to understand why the focus of a Just Culture is on the system. Rather than just blaming the person who actively made the mistake, it draws attention to the latent conditions – the holes in the cheese slices – that made that mistake possible or facilitated in the first place and are the real causes of mistakes. A Just Culture aims to identify and address these systemic vulnerabilities to prevent future incidents. Error management in the healthcare sector plays a central role in this and is essential for improving safety barriers.
Just Culture: Essential for Patient Safety and Error Management in Healthcare
In the highly complex Swiss healthcare system, characterized by time pressure and scarce resources, a Just Culture is particularly important. A traditional blame culture leads employees to remain silent for fear of reprisals. Risks remain undetected, mistakes are repeated. A study by the Swiss Patient Safety Foundation shows that only about half of professionals express safety concerns, often due to hierarchies or resignation (Leibold & Fridrich, 2024).
A Just Culture turns this approach around:
- It promotes open reporting: Through the psychological safety it creates for employees, they dare to report near misses and unsafe conditions (e.g. via anonymous reporting systems such as CIRS – Critical Incident Reporting System) – valuable information that would otherwise be lost.
- It enables learning: Reported events can be analyzed to uncover and remediate systemic vulnerabilities.
- It assigns responsibility fairly: It differentiates between human error, risky behaviour and reckless action and enables appropriate reactions.
- It strengthens the safety culture: It is a foundation for a proactive safety culture in which safety is understood and lived as a shared value.
The benefits are clear: increased patient safety, more motivated teams, and even cost savings, as up to 13% of direct hospital costs are attributable to quality and safety issues, according to the OECD (2024). This highlights the importance of error management in healthcare, which can both reduce costs and improve the quality of care.
A question of perspective: safety culture instead of error culture and the role of error management in healthcare
Interestingly, PD Dr. med. Sven Staender, pioneer of patient safety in Switzerland and co-founder of CIRS, is critical in this regard and advocates speaking of a safety culture, learning culture or improvement culture rather than an “error culture” or “blame culture”. “The term error culture suggests that people are the problem. Instead, we should consider employees as part of security,” he emphasizes in an interview with new-win (2025). When something happens, Staender says, the question should be, “Why did it happen and what can we learn from it?” instead of assigning blame. This perspective underlines the positive, learning-oriented orientation of Just Culture.
PD Dr. med. Sven Staender, who co-developed the first CIRS at the University Hospital Basel in 1995 and, as a partner of new-win, supports the dissemination of modern reporting systems such as H-CIRS (web-based reporting system for critical events), brings more than 30 years of experience in this field. His vision: Healthcare facilities that learn from mistakes instead of making them taboo (new-win, 2025). A vivid practical example from his time as chief physician at Männedorf Hospital is the “marching stop” before operations – a brief pause by the team to check whether everything is correct. Such simple but effective measures, combined with open communication, can prevent mishaps (SRF, 2020). Error management in the healthcare sector is essential to establish and optimize such preventive measures.
Just Culture in Switzerland: Where do we stand?
Although the principles of Just Culture are internationally recognised, there is still no explicit national anchoring of Just Culture in the healthcare system in Switzerland through laws or binding guidelines, as the feasibility study by the Swiss Patient Safety Foundation on behalf of the Federal Quality Commission (EQK) found. The study was intended to clarify whether and how a Just Culture can be implemented in the Swiss healthcare system. It confirms the feasibility but also highlights challenges such as hierarchies, time pressure and the lack of uniform definitions and recommends targeted training, clear responsibilities and the promotion of anonymous reporting systems. Particular emphasis is placed on the recommendation that the federal government should examine or support the legal anchoring of Just Culture in order to strengthen patient safety across the board and meet the legal requirements for quality management (Leibold & Fridrich, 2024).
Implementation has so far been inconsistent. While some hospitals are pioneering work, others are still in their infancy or are struggling with a deep-rooted culture of blame. Modern tools such as new-win’s H-CIRS system could provide decisive support here by enabling anonymous reports, structured analyses and integration into quality management, thus making Just Culture a lived practice. Error management in healthcare is crucial to this process and must be systematically promoted.
Outlook: The series continues
Just Culture is more than just a buzzword – it is the foundation for safe, trustful and learning-oriented healthcare. By overcoming the blame culture and seeing mistakes as an opportunity, we can increase patient safety, increase employee confidence and improve the quality of care.
This is the first part of our blog series on Just Culture. In the next few articles, we’ll dive deeper: we’ll take a closer look at the different types of human behavior, discuss practical steps to implement a Just Culture in organizations, and shed light on the important role of reporting systems like H-CIRS. Error management in the healthcare sector will play a central role in this and will be decisive for the success of these measures.
References
Boysen, P. G. (2013). Just Culture: A Foundation for Balanced Accountability and Patient Safety.
The Ochsner Journal, 13(3), 400–406.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3776518/
bundesaerztekammer.de – Medication errors and the “Swiss cheese” model: serious confusion
Dekker, S. (2012). Just Culture: Balancing Safety and Accountability. Ashgate Publishing.
http://ndl.ethernet.edu.et/bitstream/123456789/20186/1/118.%20Sidney%20Dekker.pdf
Leibold, A. & Fridrich, A. (March 2024). Just Culture feasibility study in the Swiss healthcare system.
Swiss Patient Safety Foundation / FOPH.
https://www.bag.admin.ch/dam/bag/de/dokumente/kuv-leistungen/eqk/machbarkeitsstudie-just-culture-2024.pdf.download.pdf/machbarkeitsstudie-Just-culture-2024.pdf
Marx, D. (2001). Patient Safety and the “Just Culture”: A Primer for Health Care Executives.
New York, NY: Trustees of Columbia University.
https://psnet.ahrq.gov/resources/resource/1582/patient-safety-and-the-just-culture-a-primer-for-health-care-executives
Marx, D. (2007). In Conversation with… David Marx,
JD. AHRQ PSNet.
https://psnet.ahrq.gov/perspective/conversation-withdavid-marx-jd
new-win SW Solutions AG (2025). Guest contribution: Interview with PD Dr. med. Sven Staender – Pioneer of patient safety.
https://newwin.ch/blog/gastbeitrag-interview-mit-pd-dr-med-sven-staender-pionier-der-patientensicherheit/
OECD. (2024). Policy Safety. Policy sub-issue.
https://www.oecd.org/en/topics/patient-safety.html
Patient safety Switzerland. Just Culture.
https://patientensicherheit.ch/forschung-entwicklung/just-culture/
Reason, J. (1990). Human Error.
Cambridge University Press.
https://www.cambridge.org/highereducation/books/human-error/281486994DE4704203A514F7B7D826C0#overview
Reason, J. (1997). Managing the Risks of Organizational Accidents.
Ashgate Publishing.
https://www.taylorfrancis.com/books/mono/10.4324/9781315543543/managing-risks-organizational-accidents-james-reason
SRF (2020). Focus on patient safety – Lack of error culture in many Swiss hospitals.
https://www.srf.ch/wissen/gesundheit/patientensicherheit-im-fokus-fehlende-fehlerkultur-in-vielen-schweizer-spitaelern
Do you have any questions about Just Culture or would you like to learn how you can promote a positive safety culture in your organization?
Whether it is the implementation of effective reporting systems such as H-CIRS-Starter, H-CIRS Professional, the use of feedback instruments such as H-FEEDBACK Starter, H-FEEDBACK Professional and H-IDEE or further advice – new-win is happy to support you on your way to more patient safety and an open learning culture.
For in-depth insights and training on the topic, we also recommend our partner PD Dr. med. Sven Staender, the leading expert in patient safety.
Contact us for a non-binding conversation! We look forward to seeing you.